Pes Planus What You Should Expect
Overview

Fallen arches, flat feet, or Plantar fasciitis can cause pain and discomfort in the legs, feet, ankles, Achilles tendon, hips, and low back. In this video, Ron Vaughn, a sports massage therapist, and Christie Powell, a physical therapist, explain how the feet become pronated (fallen arches) and how some simple at-home exercises can strengthen the arch muscles to allevaite pain and discomfort.
Causes
Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy. You may have noticed that one common element in the conservative treatment of all types of flat feet is orthoses. Many companies now manufacture semi-custom orthotic devices that not only improve comfort, but also seek to control abnormal motion of the foot. These over-the-counter inserts, in the $25 to $50 range, are an economical treatment that may help a majority of people. Unfortunately, these semi-custom devices will not fit everyone perfectly, and those of us who differ too much from the average may respond better to custom orthotic devices. Custom inserts are prescribed by your foot and ankle specialist and are made individually from either a physical or computerized impression of your feet. The only drawback of custom orthoses is their cost, ranging anywhere from $300 to $500. Many physicians recommend trying over-the-counter inserts first (and even keep them in stock) as they may save their patients large sums of money.
Symptoms
Some people have fallen arches, and they aren?t even aware of it, fallen arches are sometimes asymptomatic and do not always cause pain. However, for others, the following symptoms may be present. Foot pain, particularly in the arches or heels, leg or back pain, feet feel tired quickly, swelling in the feet and difficulty moving the feet.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Can you fix a fallen arch?
Non Surgical Treatment
Treatment of flat feet may be appropriate if there is associated foot or lower leg pain, or if the condition affects the knees or the lower back. Treatment may include using Orthoses such as an arch support, foot gymnastics or other exercises as recommended by a podiatrist/orthotist or physical therapist. In cases of severe flat feet, orthoses should be used through a gradual process to lessen discomfort. Over several weeks, slightly more material is added to the orthosis to raise the arch. These small changes allow the foot structure to adjust gradually, as well as giving the patient time to acclimatise to the sensation of wearing orthoses. Once prescribed, orthoses are generally worn for the rest of the patient's life. In some cases, surgery can provide lasting relief, and even create an arch where none existed before; it should be considered a last resort, as it is usually very time consuming and costly.
Surgical Treatment

In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Fallen arches, flat feet, or Plantar fasciitis can cause pain and discomfort in the legs, feet, ankles, Achilles tendon, hips, and low back. In this video, Ron Vaughn, a sports massage therapist, and Christie Powell, a physical therapist, explain how the feet become pronated (fallen arches) and how some simple at-home exercises can strengthen the arch muscles to allevaite pain and discomfort.
Causes
Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy. You may have noticed that one common element in the conservative treatment of all types of flat feet is orthoses. Many companies now manufacture semi-custom orthotic devices that not only improve comfort, but also seek to control abnormal motion of the foot. These over-the-counter inserts, in the $25 to $50 range, are an economical treatment that may help a majority of people. Unfortunately, these semi-custom devices will not fit everyone perfectly, and those of us who differ too much from the average may respond better to custom orthotic devices. Custom inserts are prescribed by your foot and ankle specialist and are made individually from either a physical or computerized impression of your feet. The only drawback of custom orthoses is their cost, ranging anywhere from $300 to $500. Many physicians recommend trying over-the-counter inserts first (and even keep them in stock) as they may save their patients large sums of money.
Symptoms
Some people have fallen arches, and they aren?t even aware of it, fallen arches are sometimes asymptomatic and do not always cause pain. However, for others, the following symptoms may be present. Foot pain, particularly in the arches or heels, leg or back pain, feet feel tired quickly, swelling in the feet and difficulty moving the feet.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Can you fix a fallen arch?
Non Surgical Treatment
Treatment of flat feet may be appropriate if there is associated foot or lower leg pain, or if the condition affects the knees or the lower back. Treatment may include using Orthoses such as an arch support, foot gymnastics or other exercises as recommended by a podiatrist/orthotist or physical therapist. In cases of severe flat feet, orthoses should be used through a gradual process to lessen discomfort. Over several weeks, slightly more material is added to the orthosis to raise the arch. These small changes allow the foot structure to adjust gradually, as well as giving the patient time to acclimatise to the sensation of wearing orthoses. Once prescribed, orthoses are generally worn for the rest of the patient's life. In some cases, surgery can provide lasting relief, and even create an arch where none existed before; it should be considered a last resort, as it is usually very time consuming and costly.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Acceptable Leg Length Discrepancy After Hip Replacement
Overview
The two major categorizations of LLD are structural and functional. A third more minor category is environmental. In structural LLD there is an actual anatomical difference in the bones of the lower extremities where one side becomes shorter than the other. This type of LLD may be genetic, where the person is born in this way. In other cases it may be due to injury or infection through the growth phases of early childhood or adolescence. Some spinal abnormalities like scoliosis can also cause this condition. Functional LLD is where the bones are not the cause of difference but a muscle or pelvic condition has the effect of weakening the leg on one side. Conditions that can cause this are muscle inflexibility, adduction contractures and pelvic obliquity (amongst others). The third less severe category of environmental LLD is caused by discrepancies in the surface that the feet and legs are resting or walking on. Banked, uneven or curved surfaces can all cause environmental LLD. In LLD the asymmetric nature of the legs in relation to hips and back caused the centre of gravity to shift from its natural position. This then results in the body attempting to compensate by either tilting the pelvic areas towards the shorter side, increased knee flexing on the longer side, flexion of the ankle plantar and foot supination towards the shorter side.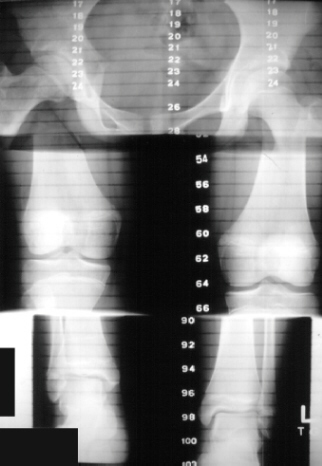
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Whether or not treatment should be pursued depends on the amount of discrepancy. In general, no treatment (other than a heel life, if desired) should be considered for discrepancies under two centimeters. If the discrepancy measures between two and five centimeters, one might consider a procedure to equalize leg length. Usually, this would involve closure of the growth plate on the long side, thereby allowing the short side to catch up; shortening the long leg; or possibly lengthening the short leg.

leg length discrepancy measurement
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
The two major categorizations of LLD are structural and functional. A third more minor category is environmental. In structural LLD there is an actual anatomical difference in the bones of the lower extremities where one side becomes shorter than the other. This type of LLD may be genetic, where the person is born in this way. In other cases it may be due to injury or infection through the growth phases of early childhood or adolescence. Some spinal abnormalities like scoliosis can also cause this condition. Functional LLD is where the bones are not the cause of difference but a muscle or pelvic condition has the effect of weakening the leg on one side. Conditions that can cause this are muscle inflexibility, adduction contractures and pelvic obliquity (amongst others). The third less severe category of environmental LLD is caused by discrepancies in the surface that the feet and legs are resting or walking on. Banked, uneven or curved surfaces can all cause environmental LLD. In LLD the asymmetric nature of the legs in relation to hips and back caused the centre of gravity to shift from its natural position. This then results in the body attempting to compensate by either tilting the pelvic areas towards the shorter side, increased knee flexing on the longer side, flexion of the ankle plantar and foot supination towards the shorter side.
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Whether or not treatment should be pursued depends on the amount of discrepancy. In general, no treatment (other than a heel life, if desired) should be considered for discrepancies under two centimeters. If the discrepancy measures between two and five centimeters, one might consider a procedure to equalize leg length. Usually, this would involve closure of the growth plate on the long side, thereby allowing the short side to catch up; shortening the long leg; or possibly lengthening the short leg.
leg length discrepancy measurement
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Everything You Need To Know About
Overview

Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term).
Causes
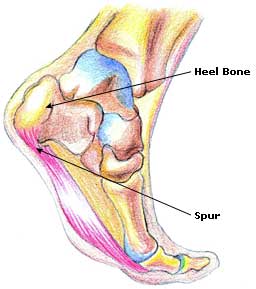
The most common cause of heel pain is a pull on the heel bone exerted by the muscles and ligaments (plantar fascia shown in illustration above) that support the arch of the foot. This is an overuse condition similar to bursitis of the shoulder or tennis elbow. Plantar fasciitis is typically very painful in the morning during the first few steps, after sitting and again at the end of the day.
Symptoms
The symptoms of plantar fasciitis are pain on the bottom of the heel, pain in the arch of the foot, pain that is usually worse upon arising, pain that increases over a period of months. People with plantar fasciitis often describe the pain as worse when they get up in the morning or after they?ve been sitting for long periods of time. After a few minutes of walking the pain decreases, because walking stretches the fascia. For some people the pain subsides but returns after spending long periods of time on their feet.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
As heel pain is basically a stress problem in the tissues of the heel, the main treatment is to reduce stress. Your doctor will advise you about weight loss and appropriate footwear. A soft heel pad is useful to wear in your shoe to act as a shock-absorber when you walk. If you have a stiff ankle or tight Achilles tendon a physiotherapist can advise on exercises for these. Stretching the Achilles tendon and plantar fascia is very effective general treatment for many patients. If you have a high-arched or flat foot, a podiatrist may advise an insole to reduce stress. Simple pain-killers such as paracetamol or anti-inflammatory medicines can help reduce the pain. Ask advice from your doctor or pharmacist before taking anti-inflammatory medicines as they can have troublesome side-effects in some people. The simple measures above will help the majority of people with heel pain. If the pain continues, a splint to wear on your ankle at night to prevent your Achilles tendon tightening up while you are asleep is often very effective in improving the severe pain that many people get first thing in the morning and breaking the cycle of pain. Your GP or an orthopaedic foot and ankle surgeon or rheumatologist may inject some steroid into the attachment of the plantar fascia to damp down the inflammation. These measures will reduce the pain in most people who are not helped by simple treatment. If you still have pain after one or two injections, your doctor may want to investigate your problem a bit further. If no other medical problem or cause of stress in your heel is found, a number of other treatments can be tried. Further physiotherapy, wearing a plaster cast to rest the inflamed tissues, pain control treatments such as transcutaneous nerve stimulation (TENS) or acupuncture. Only if all non-surgical treatments fail would an operation be considered.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
bestshoelifts
Prevention

Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term).
Causes
The most common cause of heel pain is a pull on the heel bone exerted by the muscles and ligaments (plantar fascia shown in illustration above) that support the arch of the foot. This is an overuse condition similar to bursitis of the shoulder or tennis elbow. Plantar fasciitis is typically very painful in the morning during the first few steps, after sitting and again at the end of the day.
Symptoms
The symptoms of plantar fasciitis are pain on the bottom of the heel, pain in the arch of the foot, pain that is usually worse upon arising, pain that increases over a period of months. People with plantar fasciitis often describe the pain as worse when they get up in the morning or after they?ve been sitting for long periods of time. After a few minutes of walking the pain decreases, because walking stretches the fascia. For some people the pain subsides but returns after spending long periods of time on their feet.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
As heel pain is basically a stress problem in the tissues of the heel, the main treatment is to reduce stress. Your doctor will advise you about weight loss and appropriate footwear. A soft heel pad is useful to wear in your shoe to act as a shock-absorber when you walk. If you have a stiff ankle or tight Achilles tendon a physiotherapist can advise on exercises for these. Stretching the Achilles tendon and plantar fascia is very effective general treatment for many patients. If you have a high-arched or flat foot, a podiatrist may advise an insole to reduce stress. Simple pain-killers such as paracetamol or anti-inflammatory medicines can help reduce the pain. Ask advice from your doctor or pharmacist before taking anti-inflammatory medicines as they can have troublesome side-effects in some people. The simple measures above will help the majority of people with heel pain. If the pain continues, a splint to wear on your ankle at night to prevent your Achilles tendon tightening up while you are asleep is often very effective in improving the severe pain that many people get first thing in the morning and breaking the cycle of pain. Your GP or an orthopaedic foot and ankle surgeon or rheumatologist may inject some steroid into the attachment of the plantar fascia to damp down the inflammation. These measures will reduce the pain in most people who are not helped by simple treatment. If you still have pain after one or two injections, your doctor may want to investigate your problem a bit further. If no other medical problem or cause of stress in your heel is found, a number of other treatments can be tried. Further physiotherapy, wearing a plaster cast to rest the inflamed tissues, pain control treatments such as transcutaneous nerve stimulation (TENS) or acupuncture. Only if all non-surgical treatments fail would an operation be considered.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
bestshoelifts
Prevention
Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Treating Mortons Neuroma
Overview
 Morton?s neuroma is a swollen nerve in the distal portion of the foot. The enlarged portion of the nerve represents scarring within the plantar nerve that occurs after chronic compression and/or repetitive injury. This may come about when the toes are squeezed together for too long, as can occur with the chronic use of high heels. The nerve that runs between your toes will swell and thicken. This can cause pain when walking. The symptoms of Morton?s neuroma can include burning pain in the foot, the feeling of a lump inside your foot, pain between the third and fourth toes typically but it can occur between other toes.
Morton?s neuroma is a swollen nerve in the distal portion of the foot. The enlarged portion of the nerve represents scarring within the plantar nerve that occurs after chronic compression and/or repetitive injury. This may come about when the toes are squeezed together for too long, as can occur with the chronic use of high heels. The nerve that runs between your toes will swell and thicken. This can cause pain when walking. The symptoms of Morton?s neuroma can include burning pain in the foot, the feeling of a lump inside your foot, pain between the third and fourth toes typically but it can occur between other toes.
Causes
Pronation of the foot can cause the metatarsal heads to rotate slightly and pinch the nerve running between the metatarsal heads. This chronic pinching can make the nerve sheath enlarge. As it enlarges it than becomes more squeezed and increasingly troublesome. Tight shoes, shoes with little room for the forefoot, pointy toeboxes can all make this problem more painful. Walking barefoot may also be painful, since the foot may be functioning in an over-pronated position.
Symptoms
What are the symptoms of Morton?s neuroma? A sharp or stinging pain between the toes when standing or walking. Pain in the forefoot between the toes. Swelling between the toes. Tingling (?pins and needles?) and numbness. Feeling like there is a ?bunched up sock? or a pebble or marble under the ball of the foot.
Diagnosis
Your health care provider can usually diagnose this problem by examining your foot. A foot x-ray may be done to rule out bone problems. MRI or ultrasound can successfully diagnose the condition. Nerve testing (electromyography) cannot diagnose Morton neuroma. But it may be used to rule out conditions that cause similar symptoms. Blood tests may be done to check for inflammation-related conditions, including certain forms of arthritis.
Non Surgical Treatment
Conservative treatment involves a reduction in the inflammation and removing the impingement factor. Reduction in inflammation is achieved via rest, elevation, ice, and massage with anti-inflammatory gels. Removing foot wear and and/r wearing broad type footwear would also help. Injection therapy is useful in reducing symptoms but not very successful in providing long term relief. The only time when it is most appropriate is when the cause of the space occupying object is not a neuroma but an inflamed bursa. Injection would help to relieve symptoms, and often cortisone is not even necessary.
Surgical Treatment
Surgical treatment has provided relief in some cases while poor results and surgical complications have resulted in other cases. It is believed that ligament weakness, as opposed to the pinching of nerves in the foot, may be to blame for recurrent pain in these situations. For reasons which are not fully understood, the incidence of Morton?s Neuroma is 8 to 10 times greater in women than in men.
Prevention
The best way to prevent a neuroma is by avoiding the things that cause them. Review your risk factors. If relatives have had similar problems, or if you know that you pronate or have any problem with the mechanics of your foot, talk with a podiatric physician about the correct types of shoes and/or orthoses for you. If you are not sure whether you have such a problem, the podiatric professional can analyze your foot, your stride and the wear pattern of your shoes, and give you an honest evaluation. Remember, though, that sometimes neuromas, like other conditions, can develop for no discernible reason. With this in mind, be good to your feet, and be aware of any changes or problems. Don?t wait to report them.
Morton?s neuroma is a swollen nerve in the distal portion of the foot. The enlarged portion of the nerve represents scarring within the plantar nerve that occurs after chronic compression and/or repetitive injury. This may come about when the toes are squeezed together for too long, as can occur with the chronic use of high heels. The nerve that runs between your toes will swell and thicken. This can cause pain when walking. The symptoms of Morton?s neuroma can include burning pain in the foot, the feeling of a lump inside your foot, pain between the third and fourth toes typically but it can occur between other toes.Causes
Pronation of the foot can cause the metatarsal heads to rotate slightly and pinch the nerve running between the metatarsal heads. This chronic pinching can make the nerve sheath enlarge. As it enlarges it than becomes more squeezed and increasingly troublesome. Tight shoes, shoes with little room for the forefoot, pointy toeboxes can all make this problem more painful. Walking barefoot may also be painful, since the foot may be functioning in an over-pronated position.
Symptoms
What are the symptoms of Morton?s neuroma? A sharp or stinging pain between the toes when standing or walking. Pain in the forefoot between the toes. Swelling between the toes. Tingling (?pins and needles?) and numbness. Feeling like there is a ?bunched up sock? or a pebble or marble under the ball of the foot.
Diagnosis
Your health care provider can usually diagnose this problem by examining your foot. A foot x-ray may be done to rule out bone problems. MRI or ultrasound can successfully diagnose the condition. Nerve testing (electromyography) cannot diagnose Morton neuroma. But it may be used to rule out conditions that cause similar symptoms. Blood tests may be done to check for inflammation-related conditions, including certain forms of arthritis.
Non Surgical Treatment
Conservative treatment involves a reduction in the inflammation and removing the impingement factor. Reduction in inflammation is achieved via rest, elevation, ice, and massage with anti-inflammatory gels. Removing foot wear and and/r wearing broad type footwear would also help. Injection therapy is useful in reducing symptoms but not very successful in providing long term relief. The only time when it is most appropriate is when the cause of the space occupying object is not a neuroma but an inflamed bursa. Injection would help to relieve symptoms, and often cortisone is not even necessary.
Surgical Treatment
Surgical treatment has provided relief in some cases while poor results and surgical complications have resulted in other cases. It is believed that ligament weakness, as opposed to the pinching of nerves in the foot, may be to blame for recurrent pain in these situations. For reasons which are not fully understood, the incidence of Morton?s Neuroma is 8 to 10 times greater in women than in men.
Prevention
The best way to prevent a neuroma is by avoiding the things that cause them. Review your risk factors. If relatives have had similar problems, or if you know that you pronate or have any problem with the mechanics of your foot, talk with a podiatric physician about the correct types of shoes and/or orthoses for you. If you are not sure whether you have such a problem, the podiatric professional can analyze your foot, your stride and the wear pattern of your shoes, and give you an honest evaluation. Remember, though, that sometimes neuromas, like other conditions, can develop for no discernible reason. With this in mind, be good to your feet, and be aware of any changes or problems. Don?t wait to report them.
How Shoe Lifts Cure Leg Length Difference
There are not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital indicates that you are born with it. One leg is structurally shorter compared to the other. As a result of developmental periods of aging, the brain senses the gait pattern and recognizes some variation. The human body typically adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch is not blatantly uncommon, require Shoe Lifts to compensate and ordinarily does not have a profound effect over a lifetime.

Leg length inequality goes mainly undiscovered on a daily basis, yet this issue is simply corrected, and can eradicate numerous cases of back problems.
Treatment for leg length inequality typically consists of Shoe Lifts . These are typically very inexpensive, regularly priced at below twenty dollars, in comparison to a custom orthotic of $200 or maybe more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most common condition impacting people today. Over 80 million men and women have problems with back pain at some stage in their life. It is a problem that costs companies millions each year on account of lost time and production. Innovative and improved treatment solutions are continually sought after in the hope of decreasing the economic influence this issue causes.

Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of situations Shoe Lifts are usually of very helpful. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by many experienced orthopaedic practitioners".
To be able to support the human body in a well balanced fashion, feet have got a vital function to play. Irrespective of that, it can be the most neglected zone of the body. Many people have flat-feet which means there is unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be impacted too. Shoe Lifts guarantee that the right posture and balance are restored.
Leg length inequality goes mainly undiscovered on a daily basis, yet this issue is simply corrected, and can eradicate numerous cases of back problems.
Treatment for leg length inequality typically consists of Shoe Lifts . These are typically very inexpensive, regularly priced at below twenty dollars, in comparison to a custom orthotic of $200 or maybe more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most common condition impacting people today. Over 80 million men and women have problems with back pain at some stage in their life. It is a problem that costs companies millions each year on account of lost time and production. Innovative and improved treatment solutions are continually sought after in the hope of decreasing the economic influence this issue causes.
Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of situations Shoe Lifts are usually of very helpful. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by many experienced orthopaedic practitioners".
To be able to support the human body in a well balanced fashion, feet have got a vital function to play. Irrespective of that, it can be the most neglected zone of the body. Many people have flat-feet which means there is unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be impacted too. Shoe Lifts guarantee that the right posture and balance are restored.
The Way To Identify Heel Spur

Overview
A heel spur occurs when calcium deposits build up on the underside of the heel bone, a process that usually occurs over a period of many months. Heel spurs are often caused by strains on foot muscles and ligaments, stretching of the plantar fascia, and repeated tearing of the membrane that covers the heel bone. Heel spurs are especially common among athletes whose activities include large amounts of running and jumping. Heel spurs often cause no symptoms but can be associated with intermittent pain, especially while walking, jogging, or running. Sharp pain in the heel can also be experienced when standing after sitting for a long period of time. Heel spurs can be a result of plantar fasciitis.
Causes
Heel spurs develop in some people that have a condition called plantar fasciitis, inflammation of the plantar fascia. Heel spurs form when the plantar fascia separates from the calcaneus. An abnormal bone growth, a hook-like spur, forms from calcium deposits that grow at the site of inflammation. Heel spurs are more common in middle-aged adults and people that have had plantar fasciitis for a long time. People with flat feet or high arches are vulnerable to heel spurs. Women who wear high-heeled shoes are more susceptible, as well.

Symptoms
Most of the time heel spurs present as pain in the region surrounding the spur, which typically increases in intensity after prolonged periods of rest. Patients may not be able to bear weight on the afflicted heel comfortably. Running, walking, or lifting heavy weight may exacerbate the issue.
Diagnosis
A thorough history and physical exam is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
There are many ways to treat heel spurs. Some remedies you can even do at home once a podiatrist shows you how. Heel spur treatment is very similar to treatment of plantar fasciitis. Here are a few of the most common treatments. First, your doctor will assess which activities are causing your symptoms and suggest rest and time off from these activities. Ice packs are used to control pain and reduce symptoms. Certain exercises and stretches help you to feel relief quickly. Medications that reduce inflammation and decrease pain are also used. Sometimes cortisone injections are given. Often special shoe orthotics can help to take the pressure off of the plantar fascia and reduce symptoms. Night splints that keep your heel stretched are sometimes recommended. Rarely, surgery is an option. A new treatment called extracorporeal shock wave therapy is being studied.
Surgical Treatment
Approximately 2% of people with painful heel spurs need surgery, meaning that 98 out of 100 people do well with the non-surgical treatments previously described. However, these treatments can sometimes be rather long and drawn out, and may become considerably expensive. Surgery should be considered when conservative treatment is unable to control and prevent the pain. If the pain goes away for a while, and continues to come back off and on, despite conservative treatments, surgery should be considered. If the pain really never goes away, but reaches a plateau, beyond which it does not improve despite conservative treatments, surgery should be considered. If the pain requires three or more injections of "cortisone" into the heel within a twelve month period, surgery should be considered.
Prevention
You can prevent heel spurs by wearing well-fitting shoes with shock-absorbent soles, rigid shanks, and supportive heel counters; choosing appropriate shoes for each physical activity; warming up and doing stretching exercises before each activity; and pacing yourself during the activities. Avoid wearing shoes with excessive wear on the heels and soles. If you are overweight, losing weight may also help prevent heel spurs.
What Are The Key Causes Of Inferior Calcaneal Spur

Overview
Heel spurs, or abnormal growths of the heel bone, can cause sharp pains in the heel, especially first thing in the morning and after long periods of rest. In many cases, a heel spur develops as a result of plantar fasciitis, which is the inflammation of the ligament that stretches along the bottom of the foot, from the base of the toes to the heel. In individuals who suffer from plantar fasciitis, the ligament pulls away from the heel as the foot bears weight. In an effort to stabilize the ligament, the body may produce calcium deposits, which can then develop into heel spurs.
Causes
Fctors that increase the risk of developing heel spurs include a high body mass index (BMI), regular vigorous activity, and intensive training routines or sports. Factors such as these are believed to increase the incidence of repetitive stress injuries that are associated with the formation of heel spurs. When a heel spur forms, extremely sharp pain along with the feeling that a part of the heel is trying to burst through the skin usually occurs. If left untreated, an individual may eventually begin to struggle to perform simple activities such as walking.
Symptoms
Heel spurs often cause no symptoms. But heel spurs can be associated with intermittent or chronic pain, especially while walking, jogging, or running, if inflammation develops at the point of the spur formation. In general, the cause of the pain is not the heel spur itself but the soft-tissue injury associated with it. Many people describe the pain of heel spurs and plantar fasciitis as a knife or pin sticking into the bottom of their feet when they first stand up in the morning, a pain that later turns into a dull ache. They often complain that the sharp pain returns after they stand up after sitting for a prolonged period of time.
Diagnosis
Diagnosis is made using a few different technologies. X-rays are often used first to ensure there is no fracture or tumor in the region. Then ultrasound is used to check the fascia itself to make sure there is no tear and check the level of scar tissue and damage. Neurosensory testing, a non-painful nerve test, can be used to make sure there is not a local nerve problem if the pain is thought to be nerve related. It is important to remember that one can have a very large heel spur and no plantar fasciitis issues or pain at all, or one can have a great deal of pain and virtually no spur at all.
Non Surgical Treatment
There are many temporary solutions to resolve the pain associated with irritation to the plantar ligaments. Common recommendations are ice and anti-inflammatory medications or even cortisone injections, however none of these solve the fundamental problem. To permanently resolve heel spurs you need to support and restrict the movement of the plantar ligaments. Flexible shoes will aggravate and often contribute to heel spurs. We recommend a RIGID orthotic that extends from the metatarsal heads to the heel to resolve heel spurs.
Surgical Treatment
When chronic heel pain fails to respond to conservative treatment, surgical treatment may be necessary. Heel surgery can provide relief of pain and restore mobility. The type of procedure used is based on examination and usually consists of releasing the excessive tightness of the plantar fascia, called a plantar fascia release. Depending on the presence of excess bony build up, the procedure may or may not include removal of heel spurs. Similar to other surgical interventions, there are various modifications and surgical enhancements regarding surgery of the heel.
Prevention
o help prevent heel and bone spurs, wear properly designed and fitted shoes or boots that provide sufficient room in the toe box so as not to compress the toes. They should also provide cushioning in appropriate areas to minimize the possibility of the irritation and inflammation that can lead to bone spurs in the feet. If needed, use inserts that provide arch support and a slight heel lift to help ensure that not too much stress is placed on the plantar fascia. This helps to reduce the possibility of inflammation and overstress. Wearing padded socks can also help by reducing trauma. Peer-reviewed, published studies have shown that wearing clinically-tested padded socks can help protect against injuries to the skin/soft tissue of the foot due to the effects of impact, pressure and shear forces. Also consider getting your gait analyzed by a foot health professional for appropriate orthotics. If you have heel pain, toe pain or top-of-the-foot pain, see your doctor or foot specialist to ensure that a spur has not developed.